Viral "whistleblower" plan: a regional grassroots linkage early warning network based on blockchain
Source of this article: Weiyang.com , the original title of the " Whistler " virus plan: building a regional grassroots linkage early warning network
Author: Huang Rui
On the morning of February 7, 2020, the Wuhan Municipal Government's website announced that Dr. Li Wenliang of Wuhan Central Hospital died of a new type of pneumonia and failed after all efforts. We express our deep condolences and regret! Pay tribute to his adherence to the front line to fight the epidemic, and sincere condolences to his family!
The author was distressed to hear this news. In this Wuhan new coronavirus incident, Dr. Li Wenliang took the lead in issuing an early warning on the Internet, and still insisted on the frontline of the epidemic to treat patients. It was heartbreaking because of public office. Called by netizens: the "whistleblower" of the virus.
- Popular science | How to design Optimistic Rollup to achieve sustainable expansion and decentralization?
- Research Report | The biggest hidden danger of blockchain security in 2020 is it
- Business Insider predicts that Libra will not be officially released in 2020, and China will release digital currency
The author has carefully read about the deeds of Dr. Li Wenliang. Dr. Li Wenliang is not a hero, but a mortal who stepped forward at a critical moment. When he released the SARS warning message on the Internet, he did not pass official channels and had limited influence, but it was Li Wenliang , Liu Wen, Xie Linka and other 8 doctors (some say 4 doctors) launched the early public awareness of the first wave of the epidemic. What is even more valuable is that these doctors are currently fighting on the front line of the epidemic. Dr. Li Wenliang left us today, but as a "whistler" of the virus, it will always be remembered for my generation.
As of February 8, 2020, 34,662 cases of coronavirus were confirmed in Wuhan, 27,657 were suspected, 723 were dead, and 2213 were cured. Since the first patient was admitted to Wuhan Jinyintan Hospital on December 1, 2019, it has affected a full 70 days, and the author has stayed at home for 17 days. Everyone may be thinking that if the warnings of Li Wenliang, Liu Wen, Xie Linka and other doctors on December 30 could attract the attention of the relevant government and departments, there would not be so many loved ones, and the virus would not cover every province. . But the reality is no, Li Wenliang, Liu Wen, and Xie Linka are also mortals. They are just like us contributing their individual strength in the actual epidemic. In the article "Improving the National Infectious Disease Surveillance and Early Warning Network with Blockchain Technology", the author discussed in depth the reasons why our national infectious disease network direct reporting and early warning system was not activated in this outbreak. I would like to further elaborate on the future More infectious diseases such as Li Wenliang, Liu Wen, Xie Linka and other "whistlers" are needed in the surveillance and early warning system of infectious diseases. They may be living people or machines, codes and systems. We need to use automation and systems. Construction of a system to achieve autonomy of epidemic prevention surveillance instead of rule of man.
The author gives two key stages of the outbreak to analyze our lack of early warning of new infectious diseases:
Phase 1: Confirmation of pneumonia of unknown cause (December 1 to December 31)
Stage 1: Confirmation of pneumonia of unknown origin
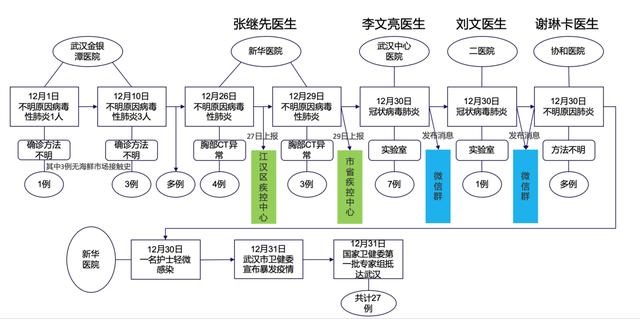
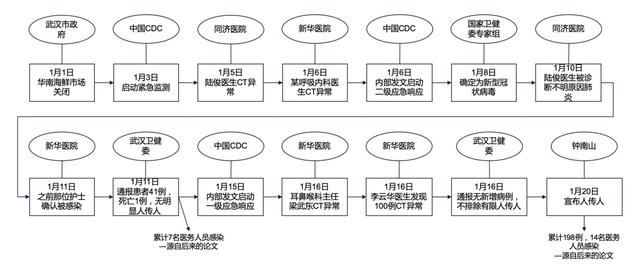
The author has organized the key timeline of the first stage for your reference. To put it simply, Wuhan Jinyintan Hospital accepted the first patient who later proved to be a new type of coronavirus pneumonia, and subsequently received several patients. Before December 26, the disease did not receive the attention of the CDC. The first abnormality was discovered by Dr. Zhang Jixian of Xinhua Hospital (Integrated Traditional Chinese and Western Medicine Hospital of Hubei Province). On December 26, 4 patients with similar symptoms were admitted. Chest CT was abnormal. Dr. Zhang Jixian reported to the Jianghan CDC on December 27. The situation. This is why Dr. Zhang Jixian is the first person to report the epidemic, not Dr. Li Wenliang. Unlike Dr. Li Wenliang's voice on the Internet, Dr. Zhang Jixian chose the official channel. On December 29, as three more similar cases were received, a total of 7 patients with unexplained pneumonia, Xinhua Hospital felt that it was a significant matter and decided to report to Wuhan and Hubei Provincial Centers for Disease Control and Prevention. On December 30, Wuhan Central Hospital, Second Hospital, and Union Hospital successively received patients with unexplained pneumonia. Wuhan Central Hospital commissioned a third-party virus test result to be similar to the SARS virus. This is also the initial reason for Dr. Wenliang Li's WeChat group alert. On the same day, Dr. Liu Wen and Dr. Xie Linka also learned the danger of the virus through their respective channels and alerted them in their respective WeChat groups. On the same day, a nurse at Xinhua Hospital developed a mild symptomatic infection. On December 31, the Wuhan Municipal Health Commission announced the outbreak, and the first batch of experts from the National Health Commission arrived in Wuhan for investigation.
The above is a brief review of the first stage. It is not difficult to see that the District Centers for Disease Control and Prevention received the epidemic report from Xinhua Hospital on December 27th. The folks first learned about it through WeChat on December 30th, and the author also found it on Wechat group on December 30th, but The author did not feel too serious at that time, thinking that it was just a case.
The next question is: The local hospital in Wuhan first admitted the patient on December 1st, the CDC received the report on December 27th, and the Wuhan Municipal Health Commission announced the epidemic on December 31st. What have we done in these 31 days?
Please see the figure below:
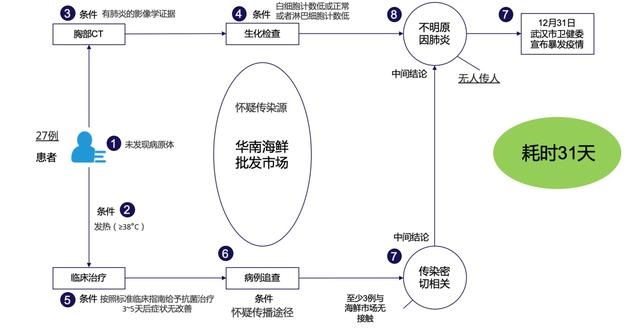
Outcome of Phase I: Announcing an outbreak without humans
As of December 31, several hospitals in Wuhan have admitted about 27 patients with unexplained pneumonia. The basic manifestations are as follows: in order to find the fever of the pathogen above 38 degrees, the image is ground glass-like, the white blood cell count is low or normal, or the lymphocyte count Low similar clinical symptoms and biochemical indicators. Based on the patient's inquiry about the exposure history, the major suspected source of infection was the South China Seafood Market, but no direct human-to-human evidence was found.
The most important result of the first stage was actually the attention of the National CDC. The first group of experts from the National Health Commission arrived in Wuhan to investigate the unknown cause of pneumonia. Therefore, in the first phase of the battle, we are still in the stage of attention and investigation. There are no specific measures for early warning and epidemic control. We have lost the key point to effectively control the epidemic in the first time.
Phase 2: Confirmation of human-to-human transmission of the new coronavirus (January 1-January 24)
Phase 2: Confirmation of new coronavirus and human-to-human transmission
From the above picture, we can see that in the second stage, the South China Seafood Market was closed on January 1; China's CDC started emergency monitoring on January 3; On January 5 and January 6, doctor infections and CT abnormalities occurred in Tongji Hospital and Xinhua Hospital, respectively. ; On January 6th, China CDC initiated a secondary emergency response; On January 8th, experts from the National Health Commission successfully isolated a new type of coronavirus and determined that the virus was the pathogen of pneumonia of unknown origin; On January 10th, Dr. Lu Jun of Tongji Hospital was diagnosed as unknown Causes of pneumonia; January 11th, Xinhua Hospital nurses who had a mild infection confirmed on December 30th; 41 cases were notified by the Wuhan Health and Medical Commission on January 11th, with no apparent human-to-human transmission; January 15th, China's CDC started level one Emergency response; On January 16, two doctors were found to have abnormal CT, and at the same time, the Wuhan Health Commission reported that there were no new cases, and human transmission was not ruled out. On January 20, Zhong Nanshan announced that human transmission of the new coronavirus has occurred, and there have been 198 cases. Patients and 14 medical staff were infected; on January 24, Hubei Province initiated a first-level emergency response after Zhejiang, Guangdong, and Hunan, which really started the comprehensive epidemic control in the province and even the whole country. It is clear to everyone that the provinces have been infected by the returning people, and no province has survived. What did our CDC do in this crucial 24 days? Any results?
See the figure below:
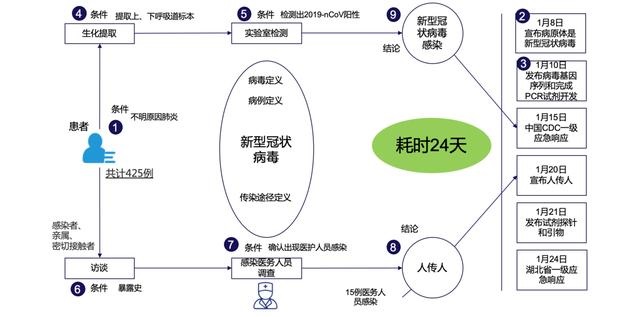
Achievements of the second stage: Isolate the virus, publish the gene sequence, complete the PCR reagents, discover human-to-human transmission, publish reagent probes and primers
In the second stage, 24 days, a total of 444 confirmed cases were reported. Here we need to pay attention to the release of probes and primers on January 21, so the confirmed cases are very different from the actual. A large number of infected people have already flowed across the country at this time. We The last key point for effective epidemic control has been lost. Of course, in the second stage, we are not without results. The results are: successful virus isolation, gene sequence release, PCR reagent release, reagent probes and primers released, and finally infection by medical staff confirmed the virus-to-human transmission and started. First-level emergency response.
Why should I spend half of my time reviewing 55 days before January 24? It is because the author believes that we have missed the best time for two outbreak warning and control.
For the first time, on December 30, Hubei Province and Wuhan City received reports from Xinhua Hospital for disease control. At the same time, multiple hospitals treated multiple patients with unknown pneumonia at the same time, and some hospitals commissioned a third party to analyze the virus. The results were similar to SARS. , There are doctors to warn on the Internet;
The second time on January 5th, due to the onset of Dr. Lu Jun of Tongji Hospital, CT showed: ground glass-like shadows, similar to other patients with unknown pneumonia, indicating that the possibility of transmission from person to person is very high.
After watching the episode of the epidemiological scientist Zeng Guang (the first group of experts to Wuhan) in an interview with CCTV on January 29, the author talked about the incident of Li Wenliang (the virus whistleblower) and felt some problems. It was praised that Li Wenliang and other 8 people were "existing Zhuge Liang", but then the words turned and they turned to Li Wenliang and other 8 people to present evidence that the virus was transmitted from person to person, because academics and public health experts are academically rigorous. I believe that the person-to-person evidence will not be available on December 30, so Li Wenliang will naturally have no chance of early warning and control of the epidemic.
Below I give my personal opinions, which are not necessarily correct but can be used for everyone to explore:
The author did not find how to define what is the evidence interpretation in the infectious disease prevention system. The author applied the requirements of evidence in the Criminal Procedure Law. The evidence can be divided into direct evidence and indirect evidence. In the absence of direct evidence, only other If the indirect evidence is true and sufficient, and can form a chain to prove the case, the defendant may be guilty and sentenced to criminal law. The author believes that epidemic prevention and control of epidemic diseases not only rely on natural sciences such as pathology and virology of infectious diseases, but also include social sciences. This is why I use the Criminal Procedure Law to describe the term evidence.
Wuhan accepted the first patient on December 1, 2019, and started a first-level emergency response on January 24, 2020. It took 55 days. Our most successful research was actually on the internal mechanism of the virus, and the pursuit was to obtain the virus. Direct evidence of infection. The first group of experts arrived in Wuhan on December 31, and completed virus isolation and confirmation on January 8 and 9 days, and then released genome sequences, PCR reagents, reagent probes and primers, and January 24 and January 27. Papers in top foreign medical journals. The speed of our research on viruses and reagents is estimated that no other country can match it! However, it is frustrating that Zhong Nanshan announced on January 20 that the virus was transmitted from human to human not through the internal research of the virus, but by the most obvious and obvious evidence: 14 medical staff were infected.
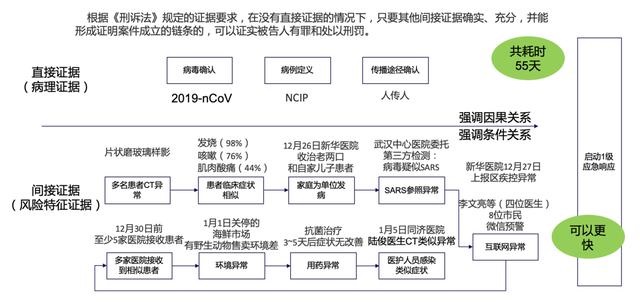
Infectious disease evidence chain
In fact, such evidence abounds. From the first patient to more and more medical staff suspected of infection, there is too much indirect evidence to form a chain of indirect evidence to prove the probability of an outbreak of a particularly serious infectious disease. Our metaphor for the pursuit of direct evidence of infectious patients is like an inappropriate analogy: you are walking in the dark night, a gangster is trying to attack you, but you can only wait until the gangster covers your mouth and exposes the knife. Waiting for direct evidence. Everyone who has had social experience knows that we can indirectly warn by observing footsteps, light, moonlight reflections, glass reflections, and the horror of the environment, etc., to prepare for escape. As a national early warning control of infectious diseases, we are concerned not only with causality, but also with conditional relations.
1. The CT of the patient is abnormal (flaky ground glass);
2. Similar clinical symptoms (fever, cough, muscle soreness);
3. On December 26, there was a collective infection in the family unit;
4. Report of suspected SARS virus appeared on December 30;
5. Doctor infection occurred on January 5 and CT abnormalities;
6. At least 5 hospitals admitted patients with unknown cause before December 30;
7. Ineffectiveness of commonly used antibacterial drugs;
8. Hygienic conditions in the seafood market;
9. and sudden vocalizations within the doctor;
If the above indirect evidence is not enough to support the whole society's early warning and escape, what we are discussing today can be said to be meaningless.
Even if you believe the author's statement, can early warning be achieved with the current system? I think the answer is also negative, and the reason is very simple. These data were not shared during the early outbreak. Although these indirect evidences are easy to find, they are scattered and difficult to record and store. Sharing between the CDC and public institutions makes it difficult to end up in a chain of evidence.
While writing this article, the author has already planned a set of regional grassroots linkage early warning network based on blockchain technology with related institutions. To commemorate Dr. Li Wenliang, he named it "the virus whistler plan". We try to build a mechanism that can separate early indirect evidence of infectious diseases from different devices, people, and institutions and encrypt distributed storage, and automatically trigger early-warning events through blockchain smart contracts, and try to replace regional governance with regional autonomy.
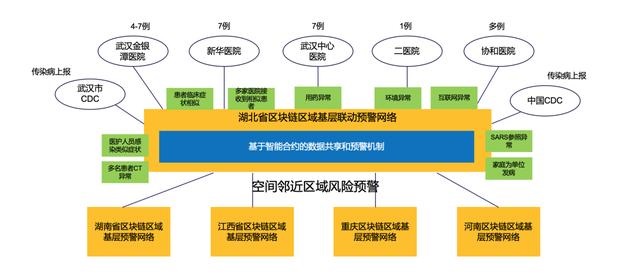
Blockchain regional grassroots linkage early warning network
Due to the spatial epidemic characteristics of infectious disease outbreaks, early regional linkage warning is very important. After the early warning contract is triggered, the proximity property of the regional epidemic prevention chain can be used (for example, the degree of adjacent areas is 1, and the degree of an interval is 2 Etc.), notify related epidemic reports of neighbouring areas, and share basic data on epidemic situation.
Relying on the ability of automatic and real-time synchronization of blockchain data, a real-time judgment and early-warning capability of data based on rule models is established through blockchain early-warning smart contracts. The current national automatic warning function for infectious diseases has been sunk into the district, city and provincial regional epidemic prevention chains to form a grassroots linkage real-time early warning network. The national top-level off-line early-warning network of infectious diseases and the real-time early-warning network at the grass-roots level work together at the same time, which can take into account both the real-time nature of the warning and the ability to predict big data.
to sum up:
This article is not a soft article promoting the blockchain. The blockchain is not a panacea, nor is it the best way to solve the problem of information transmission, but it is indeed a feasible practice of social governance, especially suitable for the basis of current medical and infectious disease prevention. Data sharing. If we automatically take out indirect evidence of infectious diseases in the early stages of the epidemic, form a chain of evidence, and put it in the hands of our government, I believe our government will choose a more early warning and control plan. This article is not to say that infectious disease pathology, viruses, and case studies are meaningless. On the contrary, I think it is very important. Patient diagnosis, treatment, and epidemic spread control all need these basic studies, but the early warning of infectious diseases requires a combination of natural science and social science. .
Finally, the author puts it: According to the interview of the Beijing News, the first batch of infected doctors in Wuhan Union Hospital was hospitalized on January 16. As the deputy director of CDC, Feng Zijian "is not particularly clear" whether the CDC received news of suspected infection by medical staff . According to him, there are many levels of data reporting, including national, provincial, municipal, and district levels. "There is a process for data reporting, and I did not understand this process in detail." This also shows that at this time the direct reporting system for infectious diseases has not been activated. Feng Zijian's explanation for this is that "pneumonitis infected by a new type of coronavirus is a new disease that does not exist in the list of infectious disease reports. Adjusting the network direct reporting system settings and personnel training require a process."
Note: Only on January 24, 2020, the National Centers for Disease Control and Prevention launched the new function of detecting new type of coronavirus pneumonia infection.
In memory of Dr. Li Wenliang! Go China! Come on in Wuhan!
We will continue to update Blocking; if you have any questions or suggestions, please contact us!
Was this article helpful?
93 out of 132 found this helpful
Related articles
- Instead of gaining weight, build a knowledge map of the blockchain in 7 days and 14 hours | Babbitt Industry Welcome Orientation
- Revisiting 2020, Bitcoin wants to say
- Compared with Bitcoin, will Ethereum be more risky in the past six months?
- Hedge funds short Zcash and XRP to hear what they say
- 22 halving coins detonated 2020: ferocious little coins, taking you to heaven and hell
- The most profitable cryptocurrency field is lending
- Overview of Cryptocurrency Market Regulation: Status, Demands, and Challenges